 "Looking beyond numbers")
The disease caused by a coronavirus called SARS-CoV-2 will have only mild illness for the majority of the population, as many medical experts opine. This means, mild Covid-19 cases can recover fully without serious medical interventions. Data on the numbers tested on Covid-19 is of utmost importance to understand the nature of the pandemic.
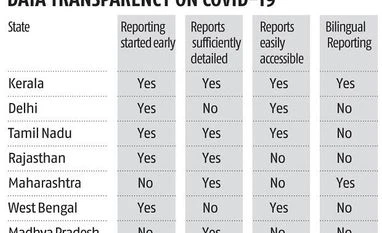
However, the reports are not easily available for many states or at the all-India level particularly on the issue of testing. Even though the data has improved in many dimensions, they are found lacking on many others. Some are not easily accessible. The state-level variations in the availability, accessibility and comprehensiveness of the data released are striking. Also, more complex information on state-wise and district-wise daily status on numbers quarantined, availability of hospital beds, ventilators, PPEs etc. is not in public domain.
Delhi, for example, released reports from the day the city reported its first case on March 4. However, data on the number of tests done, a critical number in the fight against Covid, was not given in the daily reports till March 28.
West Bengal began reporting the number of tests done from February 4, long before it saw the first case on March 17. However, suddenly from April 4, the data reporting became hazy. The number of samples sent for testing is reported, but reporting on the status of the sample, that is, whether positive or negative, has been stopped. Rajasthan saw its first case on March 14. Detailed reporting began from March 16. However, the reports are not made available on an official website and instead one has to scour Twitter accounts of journalists to get them.
Maharashtra, after starting its reporting very late, gave detailed reports with the details on the numbers tested, though only the latest report is available on the state’s website.
Madhya Pradesh, understandably, has begun releasing reports giving testing numbers only from March 30. They form part of the media bulletins that are posted on one of the state’s official Twitter handles, which makes accessing them a difficult exercise. The state health department’s website gives only limited information on any aspect of the pandemic and the “Corona Testing” page on its dashboard is still under construction.
In fact, except for Kerala and Tamil Nadu, no other major state affected by Covid-19 have released regular reports from the beginning providing comprehensive data that can be easily accessed through the website.
Reporting for all-India data at the ministry level started only from March 6. The difference between tests done and individuals tested remained constant at 890 for several days for some unexplained reason. To avoid confusion, ICMR stopped reporting the number of individuals tested, only to resume it again a week later. More importantly, only the latest report is kept available on the ICMR website. Data on state-wise numbers of tests done has never been released.
Another issue is that of language. Gujarat and Madhya Pradesh only provide reports in their state’s official language: Gujarati and Hindi respectively. Maharashtra’s reports are erratic, sometimes they are posted in both Marathi and English and sometimes in one of the two languages. Tamil Nadu, West Bengal, Delhi, Rajasthan and the ministry give reports in English only. Kerala stands out again, giving reports in both Malayalam and English always.
As of April 2, Kerala was far ahead of any other Indian state in tests per million while having lower than mean percentage of positive cases. At one point Kerala, Maharashtra and Tamil Nadu had a comparable number of cases: between 300 and 400. If the entire country was following the same rules on who should be tested (that is, testing criteria), Kerala’s testing numbers would not have been so much better than other states by now. In fact, Kerala took the lead in testing from the very beginning and has fallen a bit behind only now after its curve has begun to flatten while cases have continued to flare up in other parts of the country.
As of March 6, India had tested 3,404 individuals, including testing the entire group of 800 individuals evacuated from Wuhan. Of these, 582 individuals were tested by Kerala alone. Thus, roughly one in five individuals were tested by Kerala. Kerala is a big emigration hub but not big enough to take a 20 per cent share. Clearly Kerala tested more because it was more proactive.
Testing criteria released on March 6 stated that symptomatic individuals with travel history will be tested as well as their close contacts. On March 6, the day testing criteria was declared for the first time, the Union minister for civil aviation tweeted that universal screening had started at all international airports. However, travel advisories issued after this date continued to list specific countries from which passengers were to be screened/advised self-quarantine. On the same day, that is, March 6, Kerala also declared that it will universally screen all international passengers and newspaper reports indicated that this was implemented at Kerala’s four international airports. On March 10, Kerala declared it will screen all domestic passengers coming in at the airports in the state. On March 15, Kerala began screening all railways and buses coming from outside the state and putting people with symptoms in quarantine. No other state government appears to have taken all these measures so proactively, going beyond what was recommended by the central government.
However, on March 20, the updated testing criteria allowed for testing of people with severe symptoms. Kerala, which by now had identified a large number of people with symptoms through its proactive screening measures, was in a position to aggressively implement this updated testing criterion and the tests done per day zoomed from an average of around 170 for the 10-day period before March 20 to 400 tests per day for the 10-day period after March 20. An increase in testing is noticeable for all the major states for which data is available for this period as well. Yet, other than Rajasthan, no other state matches Kerala’s jump. Kerala had already been testing aggressively for a long time and the change in testing criteria only increased its lead on other states in tests done per million population.
Why is Kerala doing so well compared to other large states? The answers are simple: It spends the highest amount per capita on public health among all major states in India (leading to better health coverage of the population), proactive screening and testing since the very beginning of the pandemic, better economic and educational status of the state population, transparency in governance and revealing timely data for strategic decision making.
We hope that India will follow epidemiological traits as observed in other countries. Needless to state, early lockdown, steady measures on identification, isolation and testing, enhancement of infrastructure on health and research, younger age structure and economic policy measures (climatic factors or vaccination) might help India avoid huge fatality as is observed in some Western countries.
There might be state-wise differences in handling the Covid-19 pandemic, health being under state directives in India. Haziness in data release, coverage and quality of data itself prove such differentials. The pandemic peaks will be lowered over time and thus, we need continuous flow of real-time state and national surveillance data for better research and understanding.
The authors are affiliates with the International Institute for Population Sciences, Mumbai
Views are personal
virajvibhute@gmail.com; aparajita@iips.net
To read the full story, Subscribe Now at just Rs 249 a month
Already a subscriber? Log in
Subscribe To BS Premium
MONTHLY₹9/day
₹249
Renews automatically
SMART ANNUAL₹5/day
₹1699₹1999
Opt for auto renewal and save Rs. 300 Renews automatically
ANNUAL₹6/day
₹1999
What you get on BS Premium?
-
 Unlock 30+ premium stories daily hand-picked by our editors, across devices on browser and app.
Unlock 30+ premium stories daily hand-picked by our editors, across devices on browser and app. -
 Pick your 5 favourite companies, get a daily email with all news updates on them.
Pick your 5 favourite companies, get a daily email with all news updates on them. '%3E%3Cg id='Artboard-Copy' transform='translate(0 0.012)'%3E%3Cg id='_126115' transform='translate(0 0)'%3E%3Cpath id='Path' d='M17.537 1.487a.473.473 0 0 0-.467.477v12.67A2.4 2.4 0 0 1 14.7 17.06H3.3A2.4 2.4 0 0 1 .933 14.634V.966H14.587v12.29a.467.467 0 0 0 .933 0V.489a.473.473 0 0 0-.467-.477H.467A.473.473 0 0 0 0 .489V14.63a3.346 3.346 0 0 0 3.3 3.382H14.7A3.346 3.346 0 0 0 18 14.63V1.965a.467.467 0 0 0-.462-.478Z' transform='translate(0 -0.012)' fill='%23c4132a'%3E%3C/path%3E%3Cpath id='Path-2' d='M12.676 3.955a.478.478 0 1 0 0-.955H2.508a.478.478 0 1 0 0 .955Z' transform='translate(0.124 0.166)' fill='%23c4132a'%3E%3C/path%3E%3Cpath id='Path-3' d='M12.676 13H2.508a.478.478 0 1 0 0 .955H12.672a.478.478 0 1 0 0-.955Z' transform='translate(0.124 0.768)' fill='%23c4132a'%3E%3C/path%3E%3Cpath id='Shape' d='M2 6v5.371a.484.484 0 0 0 .467.5H7.531a.484.484 0 0 0 .467-.5V6a.484.484 0 0 0-.467-.5H2.467A.484.484 0 0 0 2 6Zm.933.5H7.066v4.375H2.933Z' transform='translate(0.122 0.317)' fill='%23c4132a'%3E%3C/path%3E%3Cpath id='Path-4' d='M12.321 5.5H8.967a.478.478 0 1 0 0 .955h3.354a.478.478 0 1 0 0-.955Z' transform='translate(0.517 0.317)' fill='%23c4132a'%3E%3C/path%3E%3Cpath id='Path-5' d='M12.321 8H8.967a.478.478 0 1 0 0 .955h3.354a.478.478 0 1 0 0-.955Z' transform='translate(0.517 0.467)' fill='%23c4132a'%3E%3C/path%3E%3Cpath id='Path-6' d='M12.788 10.977a.473.473 0 0 0-.467-.477H8.967a.478.478 0 1 0 0 .955h3.354a.471.471 0 0 0 .467-.478Z' transform='translate(0.517 0.617)' fill='%23c4132a'%3E%3C/path%3E%3C/g%3E%3C/g%3E%3C/g%3E%3C/svg%3E) Full access to our intuitive epaper - clip, save, share articles from any device; newspaper archives from 2006.
Full access to our intuitive epaper - clip, save, share articles from any device; newspaper archives from 2006. Preferential invites to Business Standard events.
Preferential invites to Business Standard events. Curated newsletters on markets, personal finance, policy & politics, start-ups, technology, and more.
Curated newsletters on markets, personal finance, policy & politics, start-ups, technology, and more.
Need More Information - write to us at assist@bsmail.in